This information booklet aims to provide helpful advice to people who are experiencing pain and swelling at the back of their heel.
The underlying cause may be due to the shape of your foot or how it functions, general health problems or overload/overuse injuries, in some cases the cause is unknown. Heel pain commonly produces footwear problems and a reduction in activity levels.
Diagnosis
A diagnosis can often be made by taking a medical history and examining your feet. Generally, a scan is needed to help confirm the diagnosis. The treatment options will vary depending on your specific problem and an individual treatment plan will be discussed during your consultation.
There is no direct correlation between the size of the deformity and the degree of symptoms experienced.
Common posterior heel pain problems:
Exostosis (bone) in the tendon:
This painful condition is due to a growth of bone within the Achilles tendon and is often associated with overuse and chronic pulling of the tendon on the back of the heel. This is a problem that progresses over time.
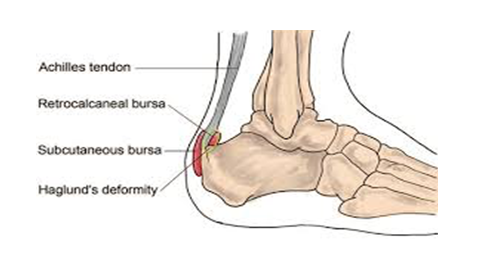
Haglund deformity:
A bony prominence on the back the heel with is often associated with a high angle of the heel bone. The prominent bony bump often irritates the bursa that sits over the bone.
Inflamed bursa:
A bursa is pocket of fluid which is found at the back of your heel. On occasions it can become inflamed and painful, but this rarely happens on its own and is usually associated with a bony problem too.
Treatment options
Conservative care
For each diagnosis, conservative care is often most helpful in the early stages of the condition. The studies suggest there is limited evidence for long term resolution of pain especially when the condition is severe.
However, conservative care is generally recommended initially and some options are listed below.
Pain medication
Comfortable supportive shoes that don’t put too much pressure on your heel.
Steroid injection (inflamed bursa)
Stretch regime for the calf muscles - these exercises can be demonstrated during your appointment or found on a YouTube video.
Orthotics - depending on your foot type you will be advised regarding a non-bespoke insole or in some cases, you will be referred to the orthotist for bespoke orthoses.
Silicone gel sheeting
Extra corporeal shockwave therapy - this treatment aims to improve healing at the tendon bone junction. This option is not available at West Middlesex University Hospital. A limited number of studies report long term success from this treatment however it appears to be more helpful when combined with calf stretch exercises.
Surgical management
If your pain continues after trying conservative care then you might consider surgery. The type of surgery will vary depending on your diagnosis. You can discuss any queries with the team and outstanding questions can be answered.
Once you are happy to proceed with surgery then, you will be asked to sign a consent form. You may need to attend a pre-surgical assessment prior to your operation and if so, an appointment letter will be sent to you.
The procedures
Bony exostosis:
The outgrowth of bone is removed from the back of your heel along with any bone that has grown into the Achilles tendon. The tendon is reattached to the bone with an anchor suture (a stitch into the bone). The inflamed bursa can be removed at the same time if required.
The incision will be closed with stitches that dissolve and a sterile dressing put on your operated foot. The procedure lasts about 45 minutes. You will wake up with bandages on your foot and a cast on your leg that goes up to your knee.
The recovery can take up to one year and depending on the quality of the Achilles tendon, the pain in your heel may persist.
Removal of bony bump:
A cut will be made towards the back of your heel near the Achilles tendon. The incision will be approximately 6 cm long and the bump of bone on your foot will be removed. Some of the Achilles tendon is detached to ensure that the bony lump has been removed, and then it is reattached.
When you wake up in the recovery area you will have bandages and an Aircast walker on your foot. You may be advised to take the boot off when resting.
Osteotomy:
A cut will be made on the side of your heel approximately 8 cm long to expose your heel bone. The bone will be cut so that a small section of bone can be removed in order to reduce the pressure at the back of your heel.
Screws are used to hold the bone together while it heals and you will be in an Aircast walker which is put on at the end of the operation. The screws normally stay in your heel bone unless they cause problems. If they do, then they can be removed which will involve another operation but generally with a much shorter recover period. There is a small chance the bones do not unite together but this is unlikely.
Bursa removal:
If an inflamed bursa is detected on your scan then it can be removed at the same time as the surgery to treat the bony outgrowth. It is unlikely you will need an inflamed bursa removed in isolation so the recovery time is dependent on the other surgeries performed.
This will mean you might be in an Aircast walker or below knee cast after the operation.
Lengthening of the calf tendon:
A tight calf muscle can cause pain at the back of your heel and this can be helped by lengthening the calf muscle. An incision is made on the back of your calf and the position will depend on the technique chosen.
The two common approaches are the Strayer or Baker. Lengthening of the tendon reduces the pull on the back of the heel but it often results in the calf muscle becoming weaker. Rarely the sural nerve is irritated leaving numbness or hypersensitivity to the lower leg.
Day Surgery
You will be admitted to the hospital and discharged on the same day. On your arrival, you will be shown to the ward and asked to change into a gown.
A member of the Podiatric surgical team will confirm your consent form, answer any remaining questions and mark the surgical site.
General anaesthetic
Prior to having a general anaesthetic, you will be reviewed by the anaesthetic team to ensure you are fit and well. You will be given all the relevant information on general anesthesia and the opportunity to ask questions.
On the day of surgery, you will be put to sleep by the anaesthetic team for the duration of our operation. A member of the podiatry team will numb your leg via a local anaesthetic injection which is given behind your knee. This injection is called a popliteal bock will be performed in the anaesthetic room before you go into the operating theatre for your surgery.
As the anatomy behind the knee varies a little from person to person, we use a nerve stimulator to locate the nerves. This sends a small electric current down the needle which stimulates the nerve. This means that the muscles controlled by the nerve begin to contract and relax causing the foot to ‘flick’. This allows us to deliver the anaesthetic with precision. Local anaesthetic at the level of the knee not only blocks sensation but also movement of your foot.
A popliteal block stops pain and movement in your foot for around 24-36 hours.
Discharge
When you leave the hospital, you will have a cast on your leg or an Aircast Walker. Depending on the type of operation you had, you will be shown how to non-weight bear or partially weight bear using crutches. Post-operative painkillers will be dispensed by the nurses along with your next appointment.
You should arrange to go home by car or taxi with an escort and have someone with you for the first 24 hours in case you feel unwell.
Reducing the risk of a blood clot (DVT)
Being in a cast and non-weight bearing after surgery places you at an increased risk of developing a DVT, if the clot travels to the lung (pulmonary embolism) this could be fatal.
You will be shown how to inject a drug (low molecular weight heparin) using a very small needle into the fat around your tummy. This thins the blood reducing the risk of you developing a DVT. The needle is very fine and for most patients it is not painful, it can leave a bruise, so we recommend that you move the injection sites around your tummy.
These injections will need to be continued whilst you are in a cast non weight bearing.
Recovery
You must rest with your leg elevated for the first 48 hours and hop using your crutches or a frame only when it is essential. Do not remove or interfere with the cast and sterile dressing underneath and it is very important to keep your leg dry.
You can buy a waterproof above knee Limbo cast cover (M100) to keep the leg dry when bathing.
Everybody recovers differently but typically you can expect the following:
Possible complications
Approximately 700 patients undergo foot surgery annually within the Department of Podiatric Surgery at West Middlesex University Hospital. Most patients have an uneventful recovery.
Outlined below are the common surgical problems or those rare complications with serious outcomes. In cases where we don’t have accurate audit we have used published results from the podiatric literature. These are accompanied by an asterisk *
Swelling taking more than 6 months to resolve occurs 1 in every 500 operations*
Haematoma – a painful accumulation of blood around the operation site. No recorded incidents.
Thick and or sensitive scar – no audit data is available.
Screw removal - this is often planned but can occur as a result of irritation.
Adverse reaction to the post-operative pain killers. 1 in every 50 patients report that the codeine preparations can make them feel sick. *
Infection of soft tissue. The incidence is 1 in every 83 operations*
Infection of bone occurred in 3 out of 916 patients.
Delayed healing of soft tissue or bone. No audit data is available.
Non-union of the osteotomy
Circulatory impairment with tissue loss occurred in 3 out of 9000 patients over a 10-year period.
Loss of sensation can occur although this is usually transient but can take up to a year to resolve.
Deep vein thrombosis which can result in a clot in the lung is potentially a life-threatening condition. Deep vein thrombosis incidence is 1 in every 900 cases.
Chronic pain syndrome: this is where the nervous system dealing with pain over reacts in a prolonged manner often to a minor incident. This normally requires management by specialists in this condition and doesn’t always resolve. This is a rare complication with no audit data available.
Reoccurrence of the problem or failure of the operation
The risk of having a complication can be minimised when the patient and all those concerned with the operation and aftercare work together. This starts with the pre-operative screening and continues through to the rehabilitation exercises.
Pre-operative screening of your health allows us to determine whether you are fit for surgery. It is important that you disclose your full medical history. If there is a query regarding your health, then further investigations or the advice of other surgical and medical specialties will be sought.
The surgeon and the theatre team will ensure that the operation is performed effectively and with the minimum of trauma.
Youcan improve the healing process and reduce the risks of complications by:
Adhering to the post-operative instructions which include resting and elevating the operated leg. Keeping the wound clean and dry until advised otherwise is essential. Please ask the nurse or Podiatric surgeon if you are not sure what to do.
Having a healthy diet is important. This provides the nutrition required for healing.
Smoking is associated with a 20% increased risk of delayed or non-healing of bones.
Alcohol can interact with the drugs that we will prescribe and in excess can impair wound healing.
Post-operative mobilisation will be advised. This helps improve the flexibility, strength and stability of your foot.
Podiatric surgeons evaluate, diagnose, prevent and treat diseases, disorders and conditions affecting the foot and all associated structures. This is carried out in keeping with the individual’s education, training and experience, in accordance with the ethics of the profession and applicable law.
Podiatric surgeons are not medical doctors.
Podiatric Surgical Training
3 year: Degree in Podiatry (BSc)
2 year: Masters in the theory of podiatric surgery (MSc)
2 year: Surgical training programme (Podiatric Surgical Trainee) Final fellowship examinations (Podiatric Surgeon)
3 year: Specialist training (Podiatric Registrar)
Accreditation with the Faculty of Podiatric Surgery