Metatarsalgia and dislocated toe deformitieshttps://www.chelwest.nhs.uk/your-visit/patient-leaflets/surgery-services/metatarsalgia-and-dislocated-toe-deformitieshttps://www.chelwest.nhs.uk/++resource++plone-logo.svg
Metatarsalgia and dislocated toe deformities
Metatarsalgia is the term used to pain affecting the ball of the foot; however it is not a diagnosis. The cause is varied and can include overuse injuries, fracture, trapped nerve, joint pain and skin lesions. The symptoms can include pain, swelling and inflammation. The problem is often worse in thin sole or high-heel shoes and aggravated by standing for long periods or lengthy walks.
Diagnosis
The effective treatment of metatarsalgia requires a thorough assessment with the treatment directed to the underlying cause or causes. This requires taking a medical history, clinically examination and investigations. Sometimes diagnostic injections of local anaesthetic are used to aid the diagnosis.
Potential causes
Gait pattern
Equinus
Foot type (cavus / pes planus)
Abnormal forefoot alignment
Inflammatory conditions
Trauma
Previous surgery
Soft tissue pathology
Skin lesions
Neuroma
Treatment options
Conservative care
The right footwear for the right occasion. When active, a firmly laced, rigid soled shoe with a cushioned inlay should be worn e.g. hiking shoes
Insoles
Strapping or toe props
Routine podiatry
Immobilisation with an Aircast Walker
Steroid injection in conjunction with the above treatments
Surgical management
Metatarsalgia
The effectiveness of your treatment over the long term will depend upon whether or not the underlying cause has been addressed when possible. Surgical options may involve a combination of procedures depending on the clinical presentation. Options can be divided into joint reconstructive procedures and joint destructive procedures
When metatarsalgia results from an abnormality in the alignment of the forefoot this can lead to overloading of the joints. The symptoms can sometimes be improved by creating an even distribution of pressure across the ball of your foot by shortening one or more of the metatarsals. The most common approach is the Weil osteotomy.
An incision is made on the top of the foot and the metatarsals are shortened and secured in the corrected position with a screw. An absorbable suture is used to close the soft tissue and skin.
After surgery the foot is placed into a post-operative shoe or Aircast walker boot for protection and aid bony healing. Post-operative stretching advice is given to reduce the risk of floating toes and stiff joints which is known risk.
Resection of the metatarsal heads
Although not common this procedure is generally selected for patients with global forefoot pain often associated with aggressive rheumatoid arthritis or severe joint deformity and malalignment.
The placement of the incision will depend on the technique used and any additional pathology. An incision can be made on either the top (dorsum) of the foot or the bottom (plantar).
Procedures for a dislocated toe
Dislocated toe(s)
This picture shows a dislocated second toe. The condition arises from when the ligaments around the joint tear or elongate as a result of trauma, chronic overloading, joint diseases or misalignment of the metatarsal lengths.
The pain generally comes from the joint or as a result of the toe rubbing against footwear. If the condition is left untreated the joint often becomes arthritic and more difficult to realign surgically.
Plantar plate repair
The diagram shows the plantar plate (ligament) intact providing approximately 30% of the stability to the toe. Once the ligament is damaged the toe comes up and the toe will start to claw.
Repairing the plantar ligament is one method of correcting the deformity. There are two approaches with a direct repair from an incision on the sole of the foot. This provides good access, but will result in a scar on the sole of the foot that can be painful.
Repairing the ligament from the top of the foot often involves cutting the metatarsal to repair the ligament and then fixing the bone. Whilst more complicated the metatarsal is often long and would need to be shortened in any case (see Weil osteotomy)
After surgery the foot is protected in an Aircast Walker boot. The risks associated with this procedure include under or over correction and joint pain if there is any wear or tear present.
Tendon transfer
This procedure is can be used to address a plantar plate injury of a hammer toe. The flexor tendon underneath the toe is released and repositioned to the top of the toe.
The tendon pulls the toe down into a corrected position and may be held in place by a screw. The risks associated with this procedure include under or over correction and occasionally the toe hyperextending.
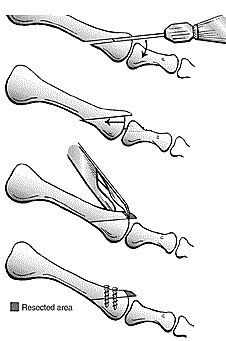
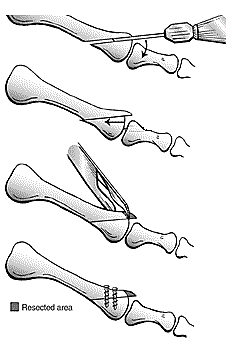
Closing wedge osteotomy
This procedure is selected when a toe deviates towards the neighbouring toe. A section of bone is removed to straighten the toe. A small wire or screw is used to hold the bone together in the corrected position and aid healing. These commonly stay in place; however, they can be removed if they cause irritation after the bone has healed.
Following surgery the foot is protected in a post-operative sandal. Risks of surgery include prolonged swelling, insufficient correction or reoccurrence of the deformity.
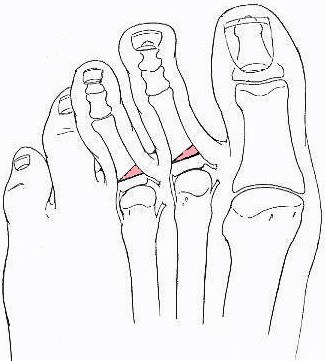
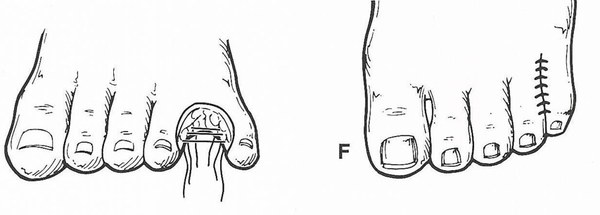
Syndactylisation of toes
This procedure is selected when the toe is dislocated and/or crosses over the neighbouring toe or the joint in the ball of the foot is damaged. The base of the toe bone is removed and sutured to the adjacent toe to correct the position and relieve pain.
After surgery the foot is placed in a post-operative sandal for two weeks. Once healed the toes should sit in a good position, however sometimes slight rotation may occur.
Amputation of toe
This procedure may be selected to provide a simple solution with a quick heeling time when complex surgery is required but inappropriate.
Following an amputation of one digit the surrounding toes can move out of alignment.
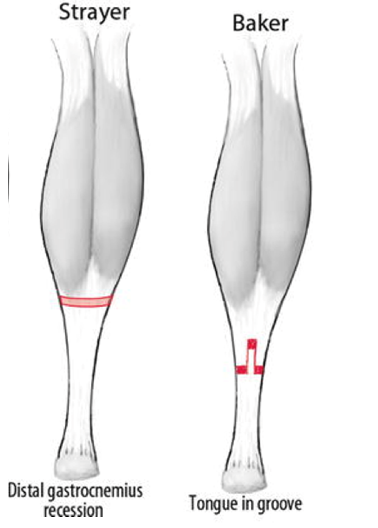
Lengthening of the calf tendon
This procedure is selected when the flexibility of the calf muscle is reduced and adversely effecting foot function and has not responded to stretching. A tight calf muscle will cause the heel to come off the ground early increasing the forces across the ball of the foot when walking.
The placement of the incision will depend on the technique. The two common approaches are the Strayer or Baker. Although lengthening the tendon allows for normal foot function the calf is often weaker and smaller than the other side after surgery. Rarely the sural nerve is irritated leaving numbness or hypersensitivity to the lower leg.
After the surgery the tendon is protected in a below the knee plaster cast and when appropriate transferred into an Aircast Walker boot.
The operation
Day surgery
You will be admitted to the hospital and discharged on the same day as your operation. On your arrival, you will be shown to the ward and asked to change into a gown. The team will confirm your consent form, answer any remaining questions and mark the surgical site (s).
Anaesthesia
You have the option of having a local (staying awake) or general anaesthetic (going to sleep). In either case the operation is normally carried out as a day case.
General Anaesthesia
On the day of your surgery, prior to having a general anaesthetic, you will be reviewed by the anaesthetic team to ensure that you are fit and well. You will be given all the relevant information on general anaesthesia and the opportunity to ask questions.
Whilst you are asleep, we will administer local anaesthetic to help reduce post-operative pain. This may last between 12 and 36 hours.
Local Anaesthesia
A member of the podiatric surgery team will anaesthetise your leg via an injection in the back of your knee (Popliteal block). This will be carried out with adequate time given to allow the local anaesthetic to take effect.
As the anatomy behind the knee may vary a little from person to person, a nerve stimulator will be used to locate the nerves. This causes the muscles to contract, causing the foot to ‘flick’. This helps us to deliver the anaesthetic with precision. Local anaesthetic at the level of the knee not only blocks sensation but also movement of your foot. This is temporary lasting for 12-36 hours.
Discharge
Before you leave the hospital, you will be given a post-operative sandal or Aircast Walker boot with or without crutches, and the nurses will show you how to use them. Post-operative painkillers will be dispensed along with your next appointment.
Recovery
You must rest with the leg elevated for the first 48 hours (essential walking only). It is important that you do not interfere with the dressings and keep them dry. You can buy a purpose made waterproof cover to keep the leg dry, from your chemist (Limbo M100 above the knee).
Full recovery takes seven to twelve months
Outcome
This type of surgery aims to redistribute the load in the forefoot and straighten the toe, allowing you to wear a greater range of footwear without discomfort.
Possiblecomplications
Approximately 700 patients undergo foot surgery annually within the Department of Podiatric Surgery at West Middlesex University Hospital. Most patients have an uneventful recovery. Outlined below are the common problems or those rare complications with serious outcomes. In cases where we don’t have accurate audit we have used published results from the podiatric literature. These are accompanied by an asterisk *
Prolonged swelling taking more than 6 months to resolve occurs 1 in every 500 operations*
Haematoma – a painful accumulation of blood within the operation site.
Thick and or sensitive scar.
Adverse reaction to the post-operative pain killers. 1 in every 50 patients report that the codeine preparations can make them feel sick.*
Infection of soft tissue. The incidence is 1 in every 83 operations*
Delayed healing of soft tissue.
Circulatory impairment with tissue loss occurred in 3 out of 9000 patients over a 10 year period.
Deep vein thrombosis which can result in a clot in the lung is potentially a life threatening condition. Within the published literature, deep vein thrombosis requiring treatment is 0.3% *
Chronic pain syndrome, this is where the nervous system dealing with pain over reacts in a prolonged manner often to a minor incident. This normally requires management by specialist in this condition and doesn’t always resolve. This is a rare complication.
Specificcomplicationsfollowingsurgery to address metatarsalgia and dislocated toes:
Insufficient correction obtained following the surgery or recurrence of deformity
Prolonged swelling of the toe
The toe may be weak or not touch the ground
Excessive shortening of the digit
The risk of having a complication can be minimised when the patient and all those concerned with the operation and aftercare work together. This starts with the pre- operative screening and continues through to rehabilitation.
Pre-operative screening of your health allows us to determine whether you are fit for surgery. Further investigations and the advice of other surgical and medical specialities will be sought as required. We will ensure that the operation is performed effectively and with the minimum of trauma.
Youcan improve the healing process and reduce the risks of complications by:
Adhering to the post-operative instructions which include resting and elevating the operated leg.
Keeping the wound clean and dry until advised otherwise is essential; please ask the team if you are not sure what to do.
Having a healthy diet is important; this provides the nutrition required for healing.
Smoking is associated with 20% increased risk of delayed or non-union of bones.
Alcohol can interact with the drugs that we will prescribe and in excess can impair wound healing.
Post-operative mobilisation when advised helps to improve the surgical outcome
Podiatric surgeons evaluate, diagnose, prevent and treat diseases, disorders and conditions affecting the foot and all associated structures. This is carried out in keeping with the individual’s education, training and experience, in accordance with the ethics of the profession and applicable law.
Podiatric surgeons are not medical doctors.
Podiatric Surgical Training
3 year: Degree in Podiatry (BSc)
2 year: Masters in podiatric surgery (MSc)
2 year: Surgical training programme (Podiatric Surgical Trainee) Final fellowship examinations (Podiatric Surgeon)
3 year: Specialist training (Podiatric Registrar)
Accreditation with the Faculty of Podiatric Surgery