Neuroma Information Leaflethttps://www.chelwest.nhs.uk/your-visit/patient-leaflets/surgery-services/neuroma-information-leaflethttps://www.chelwest.nhs.uk/++resource++plone-logo.svg
Neuroma Information Leaflet
A neuroma is an enlarged fibrous nerve in the front of the foot in-between the metatarsal bones (inter-metatarsal space). The deep transverse ligament runs across the metatarsal heads.
The nerves run in the inter-metatarsal space underneath the deep transverse ligament and divide into two digital nerves. The neuroma in the diagram is positioned in the third - fourth inter-metatarsal space.
The cause of neuromas remains unclear. Neuromas are more common in females but can affect anyone. Frequently they are found in the third - fourth inter-metatarsal space (50-70% of patients) with the second-third inter-metatarsal space being the next most common site.
Symptoms
Most patients complain of a sharp shooting pain affecting the front of their foot that radiates towards their toes. Some patients experience numbness, tingling and often describe a sensation of “walking on a stone”.
Symptoms can be initiated or made worse by wearing footwear with a narrow toe box or increased heel height, walking or driving for extended periods of time and high impact activities. Resting and removing aggravating footwear can often alleviate symptoms.
Diagnosis
A clinical diagnosis can be made via an examination and taking a through medical history, with confirmation by an ultrasound scan or MRI.
Treatment options
Surgical management
When conservative treatments fail or are unsuitable the neuroma can be treated surgically by either decompressing the nerve or removing it through an incision on the dorsal (top) or plantar (bottom) of the forefoot.
Dorsal approach
An incision will be made on the dorsum (top) of your foot over the inter-metatarsal space that the neuroma or neuromas are situated in. The incision is approximately 4cm long and can either be made in a straight line or a curved line depending again on the placement of the neuroma(s).
If there are more than one neuroma the surgeon may use a single curved incision or two parallel straight lines to access the neuromas.
A cut is made through the deep transverse ligament to access the neuroma. The neuroma is released from the surrounding soft tissue structures and removed.
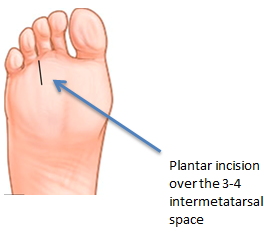
Plantar approach
An incision will be made on the plantar (bottom) aspect of your foot over the inter-metatarsal space that the neuroma or neuromas are situated in. The incision is approximately 4cm long.
Decompression
An incision will be made on the top of your foot over the inter-metatarsal space that the neuroma or neuromas are situated, as with the dorsal approach.
The deep transverse ligament is cut and the neuroma is released from the soft tissue and debrided if required. The neuroma remains in situ the aim being to elevate the pain whilst maintaining sensation.
Anaesthesia
You may have the option to have a general or local anaesthetic. The operation is normally carried out as a day case i.e. you will be admitted to the hospital and discharged on the same day.
When you arrive at the day surgery unit you will be called into the ward and clerked in by one of the day surgery team. You will change into a surgery gown and one of the podiatric surgery team will greet you.
General anaesthetic
On the day of surgery you will be put to sleep by one of the anaesthetic team for the duration of the operation. We will administer local anaesthetic around your ankle to help reduce post-operative pain.
When you wake up in the recovery wars, your foot will be numb and this will last for 12-36 hours.
Local anesthetic
A member of the podiatric surgery team will anaesthetise your leg via an injection in the back of your knee (Popliteal block). This will be carried out with adequate time given to allow the local anaesthetic to take effect.
As the anatomy behind the knee may vary a little from person to person we use a nerve stimulator to locate the nerves. This causes the muscles to contract and relax causing the foot to ‘flick’. This helps us to deliver the anaesthetic with precision. Local anaesthetic at the level of the knee not only blocks sensation but also movement of your foot. This is temporary lasting for 12-36 hours.
Discharge
Before you leave the hospital you will be given a post-operative shoe and shown how to walk using crutches. The day surgery team will dispense post-operative pain medication.
You should arrange to go home via car or taxi with an escort. You will need to have someone with you for the first 24 hours in case you feel unwell.
Recovery
You must rest with the leg elevated for the first 48 hours (essential walking only). It is important that you do not interfere with the dressings and keep them dry.
You can buy a purpose made waterproof cover to keep the leg dry, from your chemist (Limbo M100 above the knee).
Outcome
After this type of surgery you will have permanent numbness between the relevant toes. However, we hope to improve or eliminate your pain. A published departmental audit reported a 94% satisfaction rate.
Possiblecomplications
Approximately 900 patients undergo foot surgery annually within the Department of Podiatric Surgery at West Middlesex University Hospital. Most patients have an uneventful recovery.
Outlined below are the common problems or those rare complications with serious outcomes. In cases where we don’t have accurate audit, we have used published results from the podiatric literature. These are accompanied by an asterisk *
Prolonged swelling taking more than 6 months to resolve occurs 1 in every 500 operations*
Haematoma – a painful accumulation of blood within the operation site.
Thick and or sensitive scar.
Adverse reaction to the post-operative pain killers. 1 in every 50 patients report that the codeine preparations can make them feel sick.*
Infection of soft tissue. The incidence is 1 in every 83 operations*
Delayed healing of soft tissue
Circulatory impairment with tissue loss occurred in 3 out of 9000 patients over a 10 year period.
Deep vein thrombosis which can result in a clot in the lung is potentially a life threatening condition. Deep vein thrombosis requiring treatment, within the published literature, is 0.3% *
Chronic pain syndrome: this is where the nervous system dealing with pain over reacts in a prolonged manner often to a minor incident. This normally requires management by specialists in this condition and does not always resolve. This is a rare complication with no audit data available.
Specificcomplicationsfollowingneuromasurgery
Reoccurrence of symptoms.
Localised scar tissue, this normally resolves with post-operative massage or physiotherapy
The risk of having a complication can be minimised when the patient and all those concerned with the operation and aftercare work together. This starts with the pre-operative screening and continues through to the rehabilitation exercises.
Pre-operative screening of your health allows us to determine whether you are fit for surgery. It is important that you disclose your full medical history. If there is a question mark against your health then further investigations or the advice of other surgical and medical specialties will be sought.
The Podiatric surgeon and the theatre team will ensure that the operation is performed effectively and with the minimum of trauma.
You can improve the healing process and reduce the risks of complications by:
Adhering to the post-operative instructions which include resting and elevating the operated leg. Keeping the wound clean and dry until advised otherwise is essential. Please ask the nurse or a member of the podiatric team if you are not sure what to do.
Having a healthy diet is important; this provides the nutrition required for healing.
Alcohol can interact with the drugs that we will prescribe and in excess can impair wound healing.
Post-operative mobilisation will be advised, this helps improve the flexibility, strength and stability of your foot.
Podiatric surgeons evaluate, diagnose, prevent and treat diseases, disorders and conditions affecting the foot and all associated structures. This is carried out in keeping with the individual’s education, training and experience, in accordance with the ethics of the profession and applicable law.
Podiatric surgeons are not medical doctors.
Podiatric Surgical Training
3 year: Degree in Podiatry (BSc)
2 year: Masters in the theory of podiatric surgery (MSc)
2 year: Surgical training programme (Podiatric Surgical Trainee) Final fellowship examinations (Podiatric Surgeon)
3 year: Specialist training (Podiatric Registrar)
Accreditation with the Faculty of Podiatric Surgery