Management of Toe Deformitieshttps://www.chelwest.nhs.uk/your-visit/patient-leaflets/surgery-services/management-of-toe-deformitieshttps://www.chelwest.nhs.uk/++resource++plone-logo.svg
Management of Toe Deformities
An abnormally shaped toe can rub against adjacent toes or be irritated by your footwear.
Symptoms include soreness between the toes, over the prominent joint or at the tip of the toe. Hard skin or corns may form and there may be associated damage to the toenail.
Diagnosis
This is a clinical diagnosis made by the examining the foot, X-rays are not normally required.
Types of toe deformities
Causes
The exact cause may be unknown
Poorly fitting or unsupportive shoes
High or low arched foot type
Previous injury such as a fracture
Increased length of toe in comparison to adjacent toes
Older age
Medical conditions such as diabetes or rheumatoid arthritis
Genetics – it may run in families
Treatment
Conservative management options
Wider/deeper fitting footwear
Routine treatment – debridement of skin lesions as required
Padding, splints or toe props to protect from irritation
Surgical management
This involves realigning the toe to a better position. Depending on the presentation this can be achieved by a tendon transfer, removing a section of the bone (arthroplasty) or pinning the toe in a straight position (arthrodesis).
Tendon transfer
A tendon transfer involves taking a tendon from the bottom of the toe and re-routing it to the top of your toe.
The re-routed tendon then functions as a corrective force as opposed to a deforming force which stops the tendon from pulling the toe into a bent position. The tendon is sutured back onto the proximal phalanx (base of the toe) in its new position using a bone anchor suture.
The tendon used is the Flexor Digitorum Longus (FDL), which is one of two tendons with the primary role of flexing the toe towards the ground.
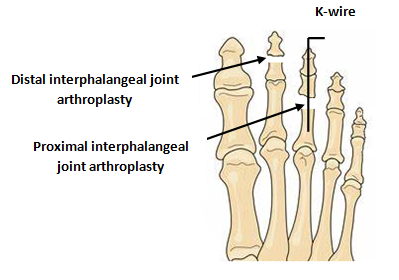
Arthroplasty
An arthroplasty is where part of the joint is removed. There are normally two joints within the toe. The type of toe deformity you have determines which joint requires the arthroplasty.
An incision is made over the top of the joint, the bone is cut, soft tissues repaired and closed with non-dissolvable sutures. The alignment may or may not be maintained with a percutaneous K wire (visible at the end of the toe) which remains in place for 4-6 weeks.
As the bones are not ‘joined together’ some mobility may remain within the toe.
Arthrodesis
Unlike the arthroplasty, an arthrodesis involves joining the bones together to give a straight but rigid toe. This may be carried out for more severe deformities; in the presence of deforming factors such as hallux valgus (bunions), hypermobility, or arthritis within the toe joint.
One or two K-wires may be used to hold the small bones in a straight position while the bones fuse together. If two wires are used, they remain inside the toe in a ‘cross’ fashion. If one wire is used, like with an arthroplasty, it is percutaneous and remains in place for 6 weeks.
A soft tissue release and tendon lengthening or repair might be required, to ensure a good position with either procedure. The choice between an arthrodesis and an arthroplasty will be made by your consultant.
Alternative procedures
An alternative, not routinely carried out in the department of podiatric surgery, is the ‘implant’ arthrodesis.
This describes the permanent application of an implant to fuse the digit in a straight position. A potential risk with this type of procedure is difficulty removing the implant in the case of irritation or revision surgery. Compared to percutaneous k-wires, which are easily removed from the end of the toe after 4-6 weeks, implant removal is more invasive and traumatic.
Recent evidence suggests there is little to no benefit in using permanent implants versus percutaneous wires, with the risk of complications being the same.
Specific complications following digital surgery:
Insufficient correction obtained following the surgery or recurrence of deformity
Prolonged swelling of the toe
The toe may be weak or not touch the ground
The pin may become loose or require early removal (if applicable)
Excessive shortening of the digit
Flail or floppy toe
Early k-wire breakage, may require revision surgery to remove the remaining wire and/or realign the digit
Additional risks associated with an arthrodesis:
The two bones may not fuse (non-union). This is not always problematic as the toe may remain straight. However, if accompanied by pain or recurrence of deformity, revision surgery may be required.
The operation
Day surgery
You will be admitted to the hospital and discharged on the same day as your operation.
On your arrival, you will be shown to the ward and asked to change into a gown. The team will confirm your consent form, answer any remaining questions and mark the surgical site (s).
Anaesthesia
You have the option of having a local (staying awake) or general anaesthetic (going to sleep). In either case the operation is normally carried out as a day case.
General Anaesthesia
On the day of your surgery, prior to having a general anaesthetic, you would be reviewed by the anaesthetic team to ensure that you are fit and well. You will be given all the relevant information on general anaesthesia and the opportunity to ask questions.
Whilst you are asleep we will administer local anaesthetic to help reduce post-operative pain. This may last between 12 and 36 hours.
Local Anaesthesia
A member of the team will anaesthetise your foot via injections. This will either be at the base of the toe which is being operated on (digital block) or in the case of multiple toes, this may be injections around your ankle (ankle block).
This can last between 12 and 36 hrs.
Discharge
Before you leave the hospital, you will be given a post-operative sandal with or without crutches, and the nurses will show you how to use them. Post-operative painkillers will be dispensed along with your next appointment.
You should arrange to go home by car or taxi with an escort. You should have someone with you for the first 24 hours in case you feel unwell.
Recovery
You must rest with the leg elevated for the first 48 hours (essential walking only). It is important that you do not interfere with the dressings and keep them dry. You can buy a purpose made waterproof cover to keep the leg dry, from your chemist (Limbo M100 above the knee).
Full recovery can take up to six months
Outcome
This type of surgery aims to straighten the toe, allowing you to wear a greater range of footwear without discomfort.
Possible complications
Approximately 700 patients undergo foot surgery annually within the Department of Podiatric Surgery at West Middlesex University Hospital. Most patients have an uneventful recovery.
Outlined below are the common problems or those rare complications with serious outcomes. In cases where we don’t have accurate audit we have used published results from the podiatric literature. These are accompanied by an asterisk *
Prolonged swelling taking more than 6 months to resolve occurs 1 in every 500 operations*
Haematoma – a painful accumulation of blood within the operation site.
Thick and or sensitive scar.
Adverse reaction to the post-operative pain killers. 1 in every 50 patients report that the codeine preparations can make them feel sick.*
Infection of soft tissue. The incidence is 1 in every 83 operations*
Delayed healing of soft tissue.
Circulatory impairment with tissue loss occurred in 3 out of 9000 patients over a 10 year period.
Deep vein thrombosis which can result in a clot in the lung is potentially a life threatening condition. Within the published literature, deep vein thrombosis requiring treatment is 0.3% *
Chronic pain syndrome, this is where the nervous system dealing with pain over reacts in a prolonged manner often to a minor incident. This normally requires management by specialist in this condition and doesn’t always resolve. This is a rare complication.
The risk of having a complication can be minimised when the patient and all those concerned with the operation and aftercare work together. This starts with the pre- operative screening and continues through to rehabilitation.
Pre-operative screening of your health allows us to determine whether you are fit for surgery. Further investigations and the advice of other surgical and medical specialities will be sought as required. We will ensure that the operation is performed effectively and with the minimum of trauma.
You can improve the healing process and reduce the risks of complications by:
Adhering to the post-operative instructions which include resting and elevating the operated leg.
Keeping the wound clean and dry until advised otherwise is essential; please ask the team if you are not sure what to do.
Having a healthy diet is important; this provides the nutrition required for healing.
Smoking is associated with 20% increased risk of delayed or non-union of bones.
Alcohol can interact with the drugs that we will prescribe and in excess can impair wound healing.
Post-operative mobilisation when advised helps to improve the surgical outcome
Podiatric surgeons evaluate, diagnose, prevent and treat diseases, disorders and conditions affecting the foot and all associated structures. This is carried out in keeping with the individual’s education, training and experience, in accordance with the ethics of the profession and applicable law.
Podiatric surgeons are not medical doctors.
Podiatric Surgical Training
3 year: Degree in Podiatry (BSc)
2 year: Masters in podiatric surgery (MSc)
2 year: Surgical training programme (Podiatric Surgical Trainee) Final fellowship examinations (Podiatric Surgeon)
3 year: Specialist training (Podiatric Registrar)
Accreditation with the Faculty of Podiatric Surgery