Laparotomy and abdominoperineal excision (APE) of the rectumhttps://www.chelwest.nhs.uk/your-visit/patient-leaflets/surgery-services/laparotomy-and-abdominoperineal-excision-ape-of-the-rectumhttps://www.chelwest.nhs.uk/++resource++plone-logo.svg
Laparotomy and abdominoperineal excision (APE) of the rectum
Information for patients, relatives and carers
This information sheet has been provided to help answer some of the questions you, your family and friends may have about laparotomy and abdominoperineal excision (APE) of the rectum (sometimes called AP resection).
What is laparotomy and abdominoperineal excision of the rectum
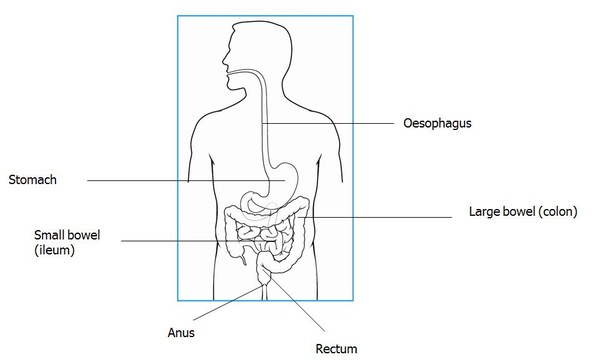
A laparotomy is the incision (cut) the surgeon makes to access the abdomen (usually a vertical line). An abdominoperineal excision of the rectum (also known as an AP resection) can then be carried out. This is an operation to remove part of the bowel that is affected by disease or is not working properly. The rectum and anal canal are removed and the opening in your bottom for wind and faeces is stitched together.
A permanent stoma (or colostomy) is also formed and, in future, your motions will pass through this stoma into a bag, as you will no longer have use of your back passage.
A stoma is an opening made on your abdomen. A piece of bowel is brought to the surface and connected to the opening, to which a bag is fitted. Faeces then passes into the bag instead of through the back passage. The stoma is red in colour but has very little sensation and is not painful. Your stoma nurse will provide you with more information.
If you had radiotherapy before the operation, the doctor may recommend that you have a type of skin graft to your bottom to help the healing process.
Alternatives to this treatment
Your doctor will discuss options with you as this will depend on your existing medical condition.
Surgery is the most common treatment for bowel cancer as it offers the best chance of cure. It may sometimes be treated with surgery and/or chemotherapy and radiotherapy.
Potential risks associated with this operation
Most people will not experience any serious complications from their surgery. The risks increase for the elderly or overweight, or people who already have other medical conditions. However, any problems that do arise can be rapidly assessed and appropriate action taken.
As with any operation, there are risks associated with having a general anaesthetic. Specific to this operation:
less than 10% risk of an adverse reaction to the anaesthetic
less than 5% risk of bleeding in the abdomen, which would require a blood transfusion
less than 5% risk of infection in the abdomen or in the wounds
less than 10% risk of obstruction (blockage) in the intestines due to scar tissue
less than 15% risk of leakage from the bowel
less than 15% risk of heart attack or pneumonia due to the general anaesthetic
less than 5% risk of blood clots (DVT or deep vein thrombosis) in the legs or lungs
less than 5% risk of accidental damage to other organs—the injury may be apparent at the time of surgery and repaired, or not known about until a few days later when further treatment may be required
Please note: Not having surgery may be a greater risk to your health than any of the risks associated with this operation.
Preparing for the operation
Before you come into hospital, try to organise things for when you return home. If you have a freezer, stock it with easy-to-prepare food. Arrange for relatives and friends to look after your children or pets, if necessary, and carry out any heavy work (such as changing bed sheets, vacuuming and gardening).
If you live alone or think you will need help at home with cooking and shopping after your operation, please tell the nurses on the ward when you are first admitted. They will then be able to help you organise this.
Please read any information that the stoma nurse has given you so that you are more prepared for the surgery. They will be able to answer any questions you have about living with a stoma.
Please arrange for someone to collect you from hospital when you are ready to go home as hospital transport is limited for exceptional circumstances.
Before the operation
A few weeks before your operation, we will ask you to attend the preassessment clinic. This appointment is an opportunity to check that you are fully prepared for your admission, treatment and discharge home. You will also have routine investigations such as blood tests, an ECG (recording of your heart), ECHO (ultrasound scan of the heart) or a chest X-ray to check you are fit for surgery.
An anaesthetist (who will be putting you to sleep for the operation) will also see you to discuss the type of anaesthetic you will have. They will also calculate how safe it is for you to proceed with the surgery and, in some cases, you may need further tests.
You will be admitted to the ward on the morning of surgery unless it is necessary for you to come in the day before. Your temperature, blood pressure, respiration rate, height, weight and urine will be checked to give the nurses a baseline (normal reading) to work with.
The stoma nurse will review you before your operation and help locate a suitable site for your colostomy (stoma). They will then visit you on the ward and support you throughout your stay in hospital. We will not expect you to look after your stoma by yourself immediately. If you need further written information about stomas, we can provide this.
You will also be given carbohydrate drinks to take before the operation to enhance your recovery. It is important that you take these and follow the instructions.
You may be advised to take laxatives before surgery—if this applies to you, it is important that you follow the instructions.
We will measure you for special stockings (known as TEDs) to prevent blood clots (DVT) from forming in your legs following surgery. We advise you to wear these throughout your stay in hospital. It is important that you move around the ward every day to reduce the risk of blood clot formation and to speed up your recovery. We may also start you on anti-coagulant (blood-thinning) injections to help minimise this risk.
On the day of the operation
The surgeon will explain the procedure to you in detail before asking you to sign a consent form, if you have not done so already. This is to make sure that you understand the risks and benefits of having the operation.
Please have a shower or bath at home before going to the operating theatre. All make-up, nail varnish, jewellery (except wedding rings, which can be taped into place), body piercings and dentures must be removed. One of the nurses will then come and prepare you for the operating theatre.
After the operation
You will wake up in the recovery room before you are taken back to the ward or the high dependency unit (HDU), depending on your medical condition before your operation. Some patients may require admission to the intensive care unit (ICU).
The section of bowel that was removed during the operation will be sent to the laboratory for testing and to confirm whether further treatment, such as chemotherapy or radiotherapy, is required. The results will be available to you about two weeks after surgery.
How will I feel after the operation?
For the first one or two days after surgery, it may be necessary to have oxygen through a mask to make your breathing easier and to reduce the risk of a chest infection. A physiotherapist will also advise you on deep breathing exercises, as well as how to move easily without discomfort.
It is important that you move about as much as possible, as this will reduce the risk of any complications and speed up your recovery. You must tell the nurse when you are in pain or feel sick. We have tablets/injections that we can give you as and when required, so that you remain comfortable and pain-free.
You may feel light-headed or sleepy after the operation—this is due to the anaesthetic and may continue until the next morning. It is also common to have a sore throat for 2–3 days after having a general anaesthetic. This sometimes happens because the anaesthetist has to pass a tube down your windpipe to give you the anaesthetic gases that keep you asleep during the operation.
The nurses will take your temperature, pulse and blood pressure at regular intervals to check your recovery. It is very important that we monitor your progress after your operation, so please be patient with the nursing staff during this time.
A catheter (tube) will be inside your bladder to drain urine away and to allow the nurses to closely monitor your urine output after the operation. The tube will be removed when your condition is stable and you are able to move around.
The dressing on your abdominal wound may be removed 24 hours after your operation and changed for a fresh dressing. Some dressings can stay on for up to a week (PICO). The nurse on the ward will look after the wound for you while you are in hospital. The wound on your bottom will also be checked daily.
After the bowel has been handled in surgery, it sometimes takes a while to start moving again. For this reason, you will not be able to have anything to eat or drink immediately after surgery. At first, you will be allowed sips of water to drink. Gradually you will be able to have other fluids and then solids. The doctors and nurses looking after you will advise you about this on a daily basis. During this time, you may have a tube in your nose which passes down into your stomach. This tube removes any excess fluid from your stomach, preventing vomiting and thereby making you more comfortable.
A ‘drip’ will also be attached to a needle in your arm or neck to provide you with fluids and prevent dehydration.
Your stoma nurse will visit you and will be happy to answer any questions you have, as well as show you how to look after your stoma.
When can I go home?
You will be in hospital for about 7–10 days, but this will depend on your recovery and the support available at home. We will discuss this with you before the operation and again while you are recovering.
Please arrange for someone to come and collect you by car on the day of your discharge home, as you will not be able to drive yourself or travel on public transport. It is important that you make the necessary plans as you will be expected to make your own arrangements for going home unless your doctor feels that there are special reasons why you need hospital transport.
We will give you a two-week supply of medication to take home with you. Any further medication will need to be prescribed by your GP. Please make sure that you arrange this before the two-week supply runs out. If you are planning your recovery away from home, you may need to register temporarily with a GP practice that is local to where you are staying.
The stoma nurse will provide you with a supply of stoma bags to get you started at home and guidance on future supplies.
Will I need to visit the hospital again?
Yes, for a check-up in the outpatient clinic 2–4 weeks after your operation. We will either give you an appointment before you leave or post one to you. Your doctor or nurse will give you the results of your operation at this appointment if you have not had them already. They will also be happy to answer any questions you have.
When can I get back to my normal routine?
Diet
There are no foods that you need to avoid after your operation. Unless you have been advised otherwise by a dietician, we recommend that you eat a well-balanced diet.
Driving
Do not drive until your strength and speed of movement are back to normal, as you must be able to perform an emergency stop. You should also make sure that you are not drowsy from any painkillers and that your concentration is good. Discuss this with your doctor if you are not sure.
It is important to inform your insurance company that you have had an operation to ensure that you are covered in the event of an accident.
Exercise and general activities
You should aim to increase your level of activity gradually. Most patients are able to get back to normal (including participating in sport or exercise) about six weeks after they go home. Simple household chores, such as vacuuming, can involve a lot of bending and stretching which you may find uncomfortable. Try to get help with this for the first 2–3 weeks after surgery.
You should not go swimming until your wound is completely healed.
If you have children, try to let them climb onto your lap when you are already sitting down, rather than lifting them up.
You should not lift anything heavier than 3 kg (6–8 lb), or roughly the weight of a full three-pint kettle, for at least two weeks.
Sexual activity
In most cases, sexual intercourse can be resumed once you have recovered from your operation and your wound is fully healed.Several things may make sex more difficult in the immediate postoperative period. Please speak to your stoma nurse who will be able to tell you about the various types of covers that are available for stomas.
Men can sometimes experience difficulties achieving an erection and may sometimes experience retrograde ejaculation (where semen goes into the bladder instead of out of your penis) because of bruising around the nerves in the pelvis. This is normally temporary and can be treated by your GP.
Some women find the shape of the vagina feels different and that it feels dry. Experimenting with different positions and using lubricants may help. It is normal to be a little anxious at first, but try to be patient. If difficulties persist, please discuss them with your doctor or nurse specialist, who will be able to help and advise.
Looking after your wounds at home
It is safe to get your wound wet, unless the doctor has told you otherwise. Please do not use antiseptic, bubble bath or anything else in the shower until the wound has healed, unless instructed by your doctor. Do not have a bath until the wound has healed.
Wash over your wound gently using soap and water, then rinse thoroughly. Pat your wound dry with a clean towel.
If your wound was closed with staples, these will need to be removed. The nurse on the ward will advise you about this before you are discharged home.
Is there anything I need to watch out for at home?
Please contact your GP or your nurse specialist if you experience any of the following:
persistent nausea (feeling sick) or vomiting (being sick)
fever or a high temperature (37.5°C/101.5°F or above)
pus (oozing) or increasing redness around either of the wound sites
increasing pain
increasing diarrhoea
Please contact your nurse specialist (details at the beginning of this leaflet) or the staff on the ward you were discharged from if you have any queries or concerns.
Contact information
Colorectal Nurse Specialists
Chelsea and Westminster Hospital T: 020 3315 8354
West Middlesex University Hospital T: 020 8321 5892