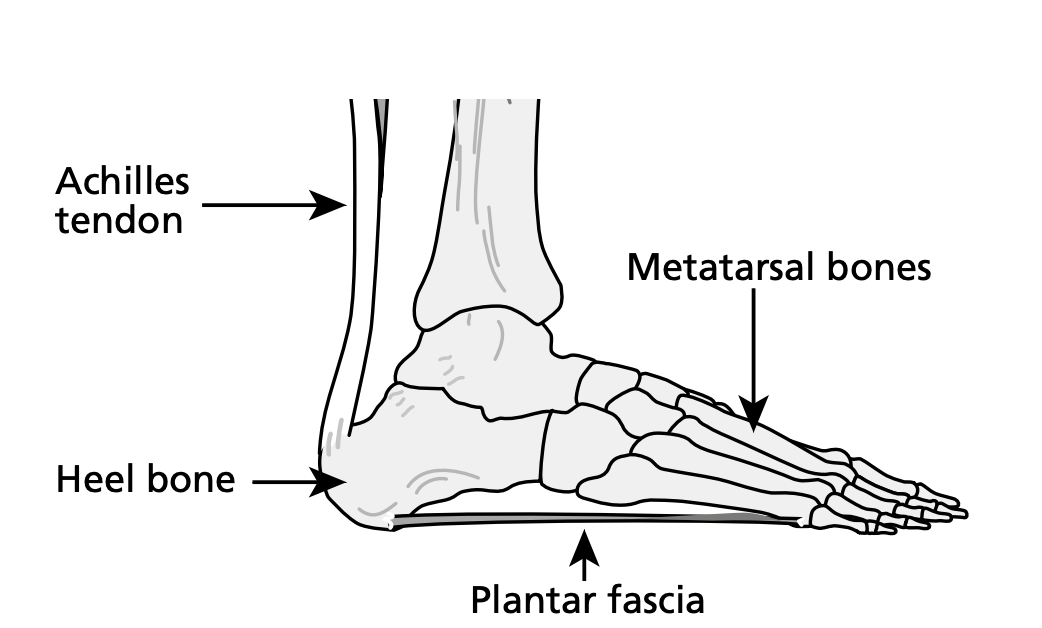
The plantar fascia is a band of thick tissue that runs along the sole of the foot. It runs from the heel bone (calcaneum) along the inside of the foot to the base of the toes. Its function is to help lift the arch of the foot when walking and act as a shock absorber for the whole leg.
What is Plantar Fasciitis?
What are the various different causes
Plantar fasciitis is a common condition that occurs when the plantar fascia becomes inflamed and irritated near where it attaches to the heel bone. Often there is a tenderness beneath the heel which can radiate into the arch of the foot.
This condition accounts for 11% to 15% of all foot symptoms referred to Foot and Ankle departments. Evidence suggests that 10% of the general population experience plantar fasciitis, with 83% of these patients being active working adults between the ages of 25 and 65 years old.
Plantar Fasciitis normally resolves within 10 months irrespective of treatment. It is classified as a chronic condition; when symptoms persist past 6 months.
What are the symptoms of Plantar Fasciitis?
Most common symptoms:
Stiffness – Stiffness and discomfort on rising in the morning or after sitting. This usually eases after a few minutes of walking. However, may last longer
Variable pain – Pain may settle during the day and with exercise, but is worse at the end of the day after periods of long standing or high levels of activity
Tenderness –Often beneath the heel bone, which can radiate into the arch of the foot
Potential causes of Plantar Fasciitis
The cause of plantar fasciitis remains unclear; however, a number of factors are known to be important:
Change or increase in activity levels
Biomechanical factors – feet which have a tendency to roll inwards/pronate
Prolonged use of flat or unsupportive footwear
Tight calf muscles
Obesity or recent weight gain – one third of those affected are overweight
Trauma
Standing for long periods on hard surfaces, causing microtrauma.
Footwear with poor cushioning or a decrease in fatty padding beneath the heel area
It can be associated with inflammatory conditions – such as psoriatic arthritis, ankylosing spondylitis and Reiter’s syndrome
Confirmation of the clinical diagnosis?
Often imaging is not necessary to make a diagnosis of plantar fasciitis; Diagnosis can usually be made by the clinician using your medical history and clinical examination.
If however it is necessary to perform imaging, an Ultrasound scan is most likely to be performed. This will be complete by the Clinical Imaging department. Ultrasound scanning is a quick, safe and effective way to see the Plantar Fascia. The scan is performed using a handheld probe, which is rolled over the skin above the plantar fascia. An image is then created by the machine and can be seen.
X-ray may show a heel spur; a small piece of bone which grows on the underside of the heel bone. This can be mistaken for the cause of plantar fasciitis. Studies suggest about 50% of symptomatic patients and 20% of asymptomatic patients have heel spurs. However, many patients with plantar fasciitis have no heel spur.
What conservative treatments are available?
Available evidence does not suggest that any of the commonly used treatments for the management of plantar fasciitis are significantly better than any other. Studies state that a combination of treatment options are effective in reducing pain and improving function.
Home treatments:
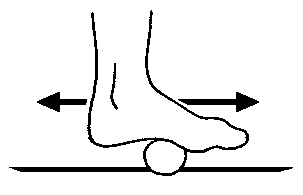
ICE:
Freeze a round bottle of water and roll it under the foot from the heel to the toes.
Reduces local inflammation
Massages and stretches the Plantar Fascia
Please take care not to apply ice for too long or directly to the skin, as this may cause ice burns.
Calf Muscle Stretching:
Tight calf muscles place extra tension on the plantar fascia and cause the feet to roll inwards/pronate.
Stretching is very important in the treatment of plantar fasciitis and can be done easily at home. A daily program of exercises to stretch your calf muscles are the mainstay of treating the condition and reducing the likelihood of reoccurrence.
How do you stretch your calf muscles?
Stand on an incline ramp or thick book:
Perform the stretch with bare feet
Stand with your toes straight or pointing towards each other slightly
Knees must be straight
If you cannot stand up straight, lower the ramp or use a thinner book
Slowly increase the height of the ramp/book as you become more flexible
Hold the stretch for 2 -5 minutes
DON’T BOUNCE
It is essential to perform these exercises twice a day. It will take approximately three months for you to become fully flexible, but you will need to continue stretching regularly to prevent a recurrence in your symptoms.
Footwear
Lace-up supportive footwear – Correct footwear to wear throughout the treatment period.
Training shoe
Hiking shoe
Benefits of this type of footwear include; help control excessive foot motion/pronation, a small heel can reduce tension on the calf muscle which may reduce symptoms AND these shoes provide the ability to use Orthotics.
Slip on, unsupportive or flat shoes – Incorrect footwear to wear throughout the treatment period.
Orthotics
Supports the arch of the foot, reducing the strain on the plantar fascia by controlling excessive pronation.
We recommend: ‘Ortha-heel’ Regular Orthotics, which can be purchased from most high street chemists for around £25 a pair or off the internet at a cheaper price. These are ¾ length insoles with a structured arch (the ‘slim-fit’ style is not suitable). These should be worn on a daily basis in lace- up shoes for maximum effect.
If your biomechanics or foot posture is considered to be the main cause of your plantar fasciitis, a member of the team may discuss a biomechanical assessment with you and custom-made orthotics.
Current evidence states that both prefabricated and custom-fitted orthotics have been shown to reduce pain and improve function in the short term with few risks or side effects.
Clinical treatment
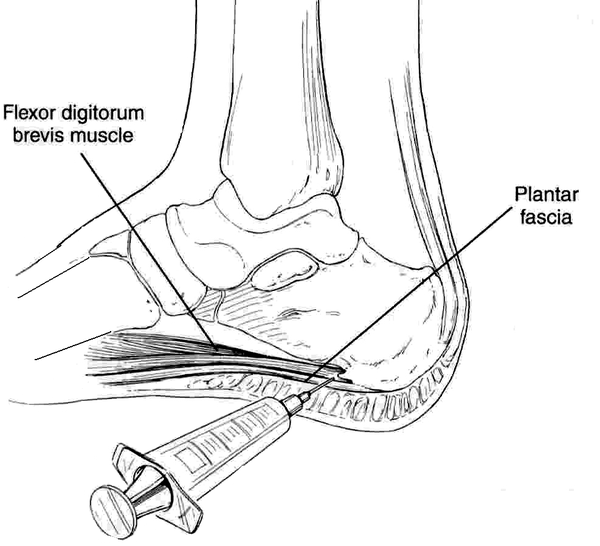
Corticosteroid Injection:
Has a strong anti-inflammatory effect which helps reduce pain locally in your heel.
Current evidence indicates that corticosteroid injections are effective for short term pain management for Plantar Fasciitis, patients who have this injection have a better short-term outcome compared with patients who do not have this treatment.
Your heel may be more painful for the first few days after the injection; this is called a ‘Flare-up’ - painkillers and ice can help reduce this discomfort. It maybe several days before you notice the benefits of the injection.
It is important to be aware of the side effects associated with this injection, side effects include thinning of the fat pad under the heel and rupture/ tear of the fascia which could cause long-lasting effects.
Nonsteroidal anti-inflammatory medication
You can use anti-inflammatory gels or tablets if appropriate (please discuss with the clinician or your GP).
Additional help
We advise that you follow the treatment plan diligently or it is unlikely your symptoms will improve.
The majority of heel pain sufferers are overweight, so dieting will be beneficial. The less you weigh, the less stress the plantar fascia is under.
If progress is slow
Night Splint: This splint maintains the foot at 90 degrees to the ankle and prevents shortening of the calf muscles and plantar fascia during sleep. This can be provided when other treatments have failed.
Physiotherapy: In some cases physiotherapy utilising soft tissue mobilisation, taping to re-align the foot, stretches, ultrasound or laser therapy can be helpful.
Surgery
This treatment option is reserved for patients who do not respond to conservative care and continue to experience unremitting pain. Tension on the plantar fascia is released by cutting through it; patients walk in a plaster cast for four weeks after surgery.
Published papers indicate that surgery may provide improvement in 48 to 86% of cases. However, research shows that patients can experience pain from other foot structures post-operatively.
Other treatments
(The hospital is unable to provide these services)
Extracorporeal Shockwave Therapy
Botulinum toxin injection
Autologous blood injection – Platelet rich plasma
Acupuncture
Podiatric surgeons evaluate, diagnose, prevent and treat diseases, disorders and conditions affecting the foot and all associated structures. This is carried out in keeping with the individual’s education, training and experience, in accordance with the ethics of the profession and applicable law.
Podiatric surgeons are not medical doctors.
Podiatric surgical training
3 year: Degree in Podiatry
2 year: Masters in the theory of podiatric surgery
2 year: Surgical training programme (Podiatric Surgical Trainee) Final fellowship examinations (Podiatric Surgeon)
3 year: Specialist training (Podiatric Registrar)
Accreditation with the Directorate of Podiatric Surgery