Thyroid and parathyroid disorders and treatmentshttps://www.chelwest.nhs.uk/your-visit/patient-leaflets/ent-audiology/thyroid-and-parathyroid-disorders-and-treatmentshttps://www.chelwest.nhs.uk/++resource++plone-logo.svg
Thyroid and parathyroid disorders and treatments
Introduction
This booklet has been designed to give you information about thyroid and parathyroid disorders and their treatments. These are two different conditions but are treated with a similar surgery. We hope it will answer some of the questions that you or those who care for you may have. This booklet is not meant to replace the discussion between you and your medical team, but aims to help you understand more about what is discussed.
What is the thyroid gland and what does it do?
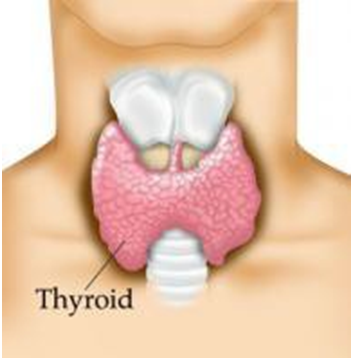
The thyroid gland is a small, butterfly-shaped gland located at the front of the neck (below the Adam’s apple). A gland is a group of cells which produces a substance such as sweat, saliva or tears. There is a variety of them all over the body.
The thyroid gland uses iodine (found in small quantities in many foods) to produce thyroid hormone which controls many aspects of health, including:
The rate at which the body’s cells work - the ‘metabolic rate’
Body weight and temperature
Heart rate and blood pressure
Mental alertness
Growth in children
If too much thyroid hormone is present in the circulation, the body’s cells will work faster than normal - this is called ‘hyperthyroidism’ i.e. the thyroid gland is overactive.
If too little thyroid hormone is in circulation, the cells will work slower than normal - this is called ‘hypothyroidism’ i.e. the thyroid gland is underactive.
What type of disorder may affect the thyroid gland?
Overactive thyroid
If your thyroid gland is overactive you may experience one or more of the following symptoms:
Restlessness
Anxiety and sleep disturbance
A fast heart rate
Increased appetite with weight loss
Diarrhoea
A dislike for hot weather
Staring eyes
Blood tests will confirm the diagnosis. You may be prescribed medication to control the effects of the excess hormone.
If the medication does not cure the disease, you may be given radioiodine treatment which involves taking a tablet. Your endocrinologist will give you information about this, and see also the patient information leaflet ‘Treatment using radioiodine’.
Surgery is another option if radioiodine and/or medication are not appropriate. The advantages and disadvantages of each option will be discussed with you by your endocrinologist and surgeon.
Underactive thyroid
If your thyroid gland is underactive you may experience one or more of the following symptoms
Tiredness
Poor appetite, weight gain and constipation
A dislike of cold weather
Swollen lips and a puffy face
Slow heart rate
Blood tests will confirm your diagnosis. An underactive thyroid is treated with medication known as ‘thyroid hormone supplementation’. These tablets are usually taken for life and levels of the hormone in your body are regularly checked with blood tests.
Goitre
When the thyroid grows so large that it becomes visible under the skin, it is called a ‘goitre’. This enlargement can occur when the thyroid is working normally, or is overactive or underactive.
A goitre is treated with surgery if it is causing problems with breathing or swallowing, or when there is a suspicion that it may be cancerous.
Thyroid tumour
Initial symptoms include a lump, a swelling in the neck, or difficulty with swallowing or breathing. Your voice may also sound different or your neck may feel uncomfortable. A thyroid tumour may be benign (non-cancerous) or cancerous.
A needle biopsy is performed (sometimes using a small amount of local anaesthetic to numb the area) to help find out whether the lump is cancerous or not. The biopsy involves a special needle which is inserted into the gland in clinic or during an ultrasound scan to obtain a small sample of cells for examination in the laboratory. In some cases, the biopsy does not provide a clear answer and it may be necessary to have an operation to remove part of the thyroid gland for a more precise examination.
If the thyroid lump is benign and not causing other trouble then it can be safely left alone. Surgery is required if the lump is cancerous.
Thyroid cancer
There are different types of thyroid cancer and your surgeon will discuss your type of cancer with you. The surgery for thyroid cancer nearly always involves removal of the entire thyroid gland (a total thyroidectomy), frequently with removal of the lymph nodes around the thyroid also – this is called a central node dissection. If the cancer has spread to other lymph nodes in your neck these may also need to be removed in a procedure known as a lateral neck dissection.
Lymph nodes are usually removed because they may contain cancer cells. Lymph nodes are also known as ‘glands’. Their main job is to help us deal with infections but they also become involved in the spread of some cancers, and may also become enlarged if this happens.
Sometime after surgery, you may be given radioiodine treatment to destroy any remaining thyroid cells. Further information about this is provided by the oncologists treating you and in the booklet ‘Treatment using radioiodine’. This combination of surgery and medical treatment is successful in curing the vast majority of patients with thyroid cancer.
Please note
Anyone that has had their entire thyroid gland removed for benign disease or cancer will need to take thyroxine tablets for the rest of their life.
What are the parathyroid glands and what do they do?
The parathyroid glands make parathyroid hormone (PTH), a substance that controls the level of calcium in your blood, which is important for the normal functioning of your muscles and nerves.
There are a minimum of four parathyroid glands, which are normally each the size of half a grain of rice. They are usually located near to the thyroid gland, but are sometimes found elsewhere in the neck or even behind the breastbone.
Overactive parathyroid
If one or more parathyroid glands become overactive (known as ‘hyperparathyroidism’), too much calcium circulates in the blood. Over time calcium loss from bones leads to the risk of fractures (broken bones) and the high levels of calcium in the blood can damage many organs including blood vessels, the kidneys, stomach, pancreas and possibly the heart. Hyperparathyroidism is diagnosed with blood tests and a urine test. It is rarely cancerous.
Treatment involves surgery (known as parathyroidectomy) by removing one or more overactive parathyroid glands. If only one gland is overactive and it can be removed easily, this may be done through a very small incision (cut). Approximately 50 per cent of patients can be treated using this method.
In other cases, where more than one gland is diseased, the diseased glands may need to be totally or partially removed. This is also usually performed through a small incision in the neck.
Overall, surgery can cure over 95 per cent of patients with hyperparathyroidism at the first operation.
Parathyroid cancer
Parathyroid cancer is rare and is treated with surgery. It may occasionally require a second operation to minimise the risk of it coming back.
What are the risks associated with thyroid and parathyroid surgery?
Thyroid and parathyroid surgery are usually performed under a general anaesthetic. Local anaesthetic operations are reserved for patients not fit enough for a general anaesthetic.
The following risks are possible after any major operations and will depend on your medical condition. However, all are uncommon in thyroid and parathyroid surgery:
Chest infection- You can help by practising deep breathing exercises and following the instructions of the physiotherapist. If you smoke, we strongly advise you to stop.
Thrombosis (blood clot in the leg)- Major surgery carries a risk of clot formation in the leg but this is uncommon in thyroid and parathyroid surgery. We encourage you to start moving around as much as you are able after surgery, and in particular regularly exercising your legs. You will be fitted with some support stockings for the duration of your stay in hospital. If you smoke, we strongly advise you to stop.
Pulmonary embolism (blood clot in the lungs)- Rarely a blood clot from the leg can break off and become lodged in the lungs. This is treated with anticoagulant (blood thinning or clot dissolving) medication. Your hospital doctor will explain more if this rare event occurs.
Specific to thyroid and parathyroid surgery there is a:
High risk of temporary neck stiffness and numbness of the skin on the front of the neck
Approximately one per cent risk of bleeding in the wound, usually within a day of surgery, which may require a second operation to resolve
Approximately one per cent risk of permanent injury to a laryngeal nerve, which may lead to a permanent hoarseness or a change in the quality of your voice. Most patients will experience a temporary change in the voice quality that usually resolves in the following days and weeks
Small risk of excessive or unsightly scarring which mainly affects those with red hair or pale and black skin
One to two per cent risk of wound infection, which rarely requires more than antibiotic treatment
Are there any alternatives to this treatment?
This will depend on your existing medical condition. Your hospital doctor will discuss the options with you if appropriate.
What will the scar be like?
Almost all patients ask about the scar resulting from surgery. Fortunately the majority of our surgery can be performed by making a small incision in the neck of 4-6 cm in length (1.5-2.5 inches).
This heals very well in the vast majority of patients. It can sometimes be difficult to see the scar once full healing has taken place, three or so months after surgery.
Are there techniques that can avoid a scar in the neck?
We have pioneered a technique in the UK using the Da Vinci robot which leaves a scar in the armpit instead of the neck. This technique cannot be recommended to all patients and is mostly appropriate for patients who have a tendency to heal poorly with thick and pigmented scars. This will be discussed with you by your surgeon. The length of hospital stay and complications are the same as in conventional surgery.
Is there anything I need to do to prepare for my operation?
If you take blood-thinning medications (such as warfarin, clopidogrel (plavix) or aspirin), we will ask you to stop taking them several days before your operation. If you are allergic to any medications, please let your hospital doctor or the ward staff know before you have your operation
Please bring your nightwear, dressing gown, slippers and toiletries with you when you come into hospital
Please bring a list of any medicines you currently take (or the medicines themselves)
Please do not bring anything valuable
Before coming into hospital
You may be sent an appointment to come to the pre-admission clinic one or two weeks before your operation. This is to make sure that you are as fit as possible for the operation and can involve some tests done, such as a blood test, chest x-ray, a heart tracing (ECG) and any other tests that may be required in your specific case.
It is essential that you come to this appointment or your operation may be cancelled.
Eating and drinking before your operation
You will usually be admitted on the day of your surgery, usually at 7.00 am. We will ask you not to eat anything six hours before and have only water until two hours before admission.
What happens before the operation?
You will probably be admitted to hospital on the day of surgery or less commonly the night before surgery. Both the surgeon and the anaesthetist will visit you.
Consent
You will be asked for your consent before the hospital staff begin your treatment. Your hospital doctor will carefully explain the procedure. Details will vary according to each individual case. No medical treatment can be given without your written consent.
If you do not understand what you have been told, let the staff know straight away, so they can explain again. You may also find it useful to write a list of questions before coming to hospital and to have a relative or friend with you to help you remember the discussion when the treatment is explained.
You will receive a copy of all communications sent to your GP, but please let us know if you prefer not to receive this.
The nurses will measure your temperature, blood pressure, breathing rate, height, weight and a urine test. A blood test may also be required.
What happens after the operation?
You will wake up in the recovery room before you are taken back to the ward where blood tests will be done to check your blood calcium level. In extensive operations or if there is some concern about your general health after surgery you may be taken to the intensive care unit for 24 hours.
How will I feel after the operation?
To reduce the possibility of puffiness in the neck we ask that you sit upright after the operation. We also ask you to sleep with the head of the bed raised slightly on the first night after the operation.
Please tell us if you are in pain or feel sick. You may experience some discomfort at the wound in your neck. Your neck may appear swollen with some numbness, which will gradually resolve as healing takes place. We have tablets and injections to give you so that you remain as comfortable and pain free possible.
After an anaesthetic you may feel light-headed or sleepy. This usually resolves in a matter of hours.
Occasionally a small drain (tube) may be left inside your wound to remove any fluid that can collect. The tube is removed when the amount of fluid collected has decreased.
You will have dissolvable stitches that do not need to be removed. Your wound is covered in biological glue which helps prevent infection and allows you to shower on the evening of surgery should you wish to do so.
You are able to take sips of water then drink fully once back on the ward after the operation. You will have a sore throat but can usually eat without too much trouble.
Often after thyroid or parathyroid surgery, the blood calcium level can fall. This will be checked regularly – on the evening of surgery and in the morning after surgery. Please tell the nurses about any feelings of tingling or numbness of the fingers, toes or around the mouth, as these can be a warning sign of low blood calcium. You may require calcium and vitamin supplements and these will be provided prior to discharge from hospital.
When can I go home?
Usually when no problems occur you will be able to go home the morning after surgery, but sometimes after larger operations you may stay two days or more.
Once you go home you must continue to take the medication as instructed to you whilst in hospital. Please take your medication as prescribed and take care not to exceed the recommended number of tablets. Repeat prescriptions can be obtained from your GP.
When can I get back to normal?
People’s recovery after operations varies greatly, but you should be able to go back to work the following week. If you do any heavy lifting or carrying at work, you may need longer to recover. Heavy exercise should be avoided for two weeks after the operation.
Will I need to visit the hospital again?
Yes. You will be given an outpatient appointment to see your surgeon and perhaps your physician. Further blood tests may be required to monitor the calcium level and your need for thyroxine tablet.
Thyroxine tablets
The removal of all the thyroid gland means that you will need to take hormone replacement tablets called thyroxine every day for the rest of your life. Thyroxine tablets are the size of a sugar sweetener and are safe to take.
It is important that you make a list of all medicines you are taking and bring it with you to all your clinic appointments. If you have any questions at all, please ask a member of your medical team. It may help to write these down as you think of them. It may also help to bring someone with you when you attend your outpatient appointments.
Information for cancer patients
We are all individuals and cope in different ways and need different lengths of time to adjust to a cancer diagnosis. Your medical team is here to support you. You may want to discuss your worries or concerns with a member of your medical team who can provide help and advice.
You may find further information from the organisations listed below.
Butterfly Thyroid Cancer Trust- This UK charity is dedicated to the support of patients with thyroid cancer. Website: www.butterfly.org.uk
AMEND- Patients with MEN (Multiple Endocrine Neoplasia) syndrome may find information on the AMEND patient support website. Website: www.amend.org.uk
Macmillan Cancer Support Helpline- This is a free helpline for people affected by cancer who have questions about cancer, need support or just someone to talk to. It is open from Monday to Friday, 9.00–20.00 (interpretation service available). Telephone: 0808 808 0000
Benefits Enquiry Line- The service provides advice and information on the range of benefits available. Telephone: 0800 88 22 00
This leaflet was created by Imperial College Healthcare NHS Trust